Laureen: Right. And you know what I want to do, I’m going to bump this question up because it’s related, asking about the CCS and CIC exams.
The CCS is the AHIMA’s certified coding specialist exam. To me, it’s one of the most comprehensive and the most difficult exams that a coder could aim for. It covers all the competencies areas. Chandra built a nice a little graphic for us. The CIC is pretty much just inpatient with a little touch about patient information.
Chandra, do you want me to pull up the slide deck or the spreadsheet or both?
Chandra: We’re going to look at both of them, but we can start with either one. All I did here with this graphic, this is actually a graphic that if you looked at any of our Blitz products, things like that, this is probably something you’ve seen somewhere along the lines; whether you took the COC and you saw me showing the difference between the CPC and the outpatient, the COC credential and how those differ. Then, when we did the CIC Blitz, I added that in and said, “OK, here’s how that differs from the pro fee side and the outpatient side. Here’s how inpatient runs.”
Then, the question was brought to me, Laureen asked me, “Can you put the CCS on there? Show us how it differs.” The reason the CCS is in purple is not only because it’s from a different organization, but it’s like comparing apples to oranges. Yes, some of the components are the same, but it’s a very different structure. You’ll notice with all of the AAPC exams, all the ones in green, the CPC, the COC, the CIC. The numbers that I have listed here are the number of questions in each section.
With the AHIMA-based CCS, it’s the percentage of total questions because their exam isn’t a set number of questions. Well, it is, but it’s so many of them are actually the test, so many of them are a pre-test and they throw those questions out, but they don’t tell you which ones they are. Depending on which version you get, it gives you a three-point window of diagnosis and procedure coding according to their candidate guide, actually it says, I think it runs from 64% to 68% of the exam; so I kind of went with the middle of the road. What average of that to 100% and was dead in the middle of whatever range they get. So, approximately 66% of the CCS exam covers diagnosis and procedure coding.
If you compare the CCS to the CIC, you’ll notice the CIC through AAPC doesn’t include any CPT coding at all. Well, the CCS does, because they include both outpatient facility and inpatient facility coding. It’s like taking the COC and the CIC and adding them together to get the CCS. That’s why I said it’s a lot more comprehensive, like Laureen said, but it is sort of apples and oranges, and they put their components in a little different group than we’re really used to. For example, they have one bucket that’s compliance but another one that is privacy, confidentiality, legal and ethical issues, where the AAPC tends to lump all of those into compliance-type things. They put the confidentiality probably up in the documentation piece. Things like that.
Then, they split their, they call theirs regulatory guidelines, reporting requirements for inpatient versus outpatient where AAPC calls them payment methodologies. It’s really kind of the same information. But the CCS also includes two additional pieces of information that are not tested on at all by AAPC.
If you can scroll up just a little bit. I want those last boxes in the CCS column. There are two areas, granted there are small percentage of the overall exam, they total 5% together, an average of 5%. But there are questions on the CCS about data quality and data management, as well as the IT side of things; IT and communications. Those are not included on the CIC or the COC for AAPC. They’re different. That’s not something that they emphasize as much.
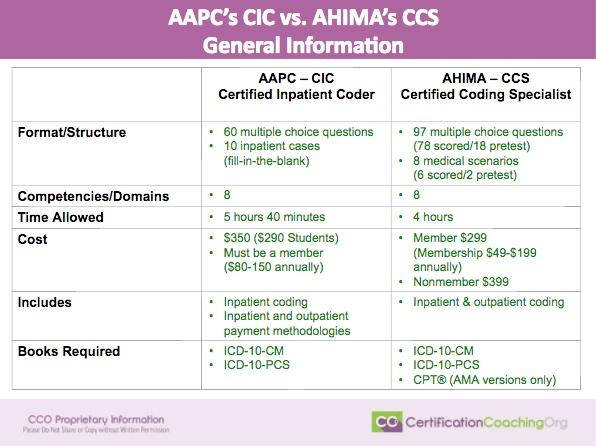
AAPC CIC vs. AHIMA CCS Exams: General Information
In the slides, what I tried to do is, I really wanted to show how different these two exams are. So, I did a couple of different visuals. I’m a very visual person. I like the graphics, I like to see the difference. I started out with – Alright, before we even get to the content of the exam, let’s talk about all the other ways that this is different. The middle column is the AAPC, which many of us, if you’ve been through training with us before at CCO, AAPC is kind of our bread and butter. That’s where most of the people that come to us are looking to get certified through the AAPC. AHIMA is the CCS, it is the column 1 on the far right.
Format/Structure – First of all, what’s the format or the structure of the exam? The CIC through AAPC is the only one of the AAPC exams to date that is not completely multiple choice questions. It is 60 multiple choice questions and then there are ten cases, all inpatient cases, that you have to code and they’re fill-in-the blanks. Yes, they tell you how many codes you need for each case. They’ll give you so many blanks and you have to have all those blanks filled in for that case. Between these two, the cases actually total between 90 and 110 codes; so if you combine those that actually put you over the total of 150 questions per se, but it’s so that you got a little wiggle room on the cases, if you don’t get everything in exactly the right order, and things like that.
The AHIMA exam is also a combination of multiple choice and coding scenarios where they tell you how many codes that you need, but theirs are 97 multiple choice questions – it’s a lot more – and two less scenarios. But the interesting thing is, they don’t score all of them and they won’t tell you which ones they’re going to score and which ones they’re not. For example, there are 97 multiple choice questions, 78 of them will be scored, 18 of them are considered pre-test and thrown out. The medical scenarios, they’re only going to score six of them and two of them are going to be considered pre-test or thrown out. Nowhere did they say that you’re too lowest, or an average or anything like that; they don’t tell you which two they’re going to disregard. So, we got similar structure but 97 is a lot more multiple choice questions than 60, but there’s two less scenarios.
Competencies/Domains – The next question becomes what kind of things are on there? Each of them has 8 domains or 8 areas of competencies, even as we saw on the Excel file, they’re not the same, they’re a little bit different. The time allowed, you get 5 hours and 40 minutes with the AAPC exam, just like you do for all of their exams, but you only get 4 hours for the AHIMA one. So, you really get to have your time down to like perfect.
Cost – AAPC you’re going to pay $425, unless you’re a student it’s going to be $325. You’ll get two attempts just like all of their other exams, but you do have to be a member to take an AAPC exam. But with AHIMA, if you’re a member, it will cost you $299 to take the exam one time. If you’re a non-member it’s going to cost you $399 to take the exam, one time. Then I gave you the membership rates; it really varies depending on what kind of a member, whether the student memberships that $49; they have like a premium membership, the $199. They’ve got a couple different in-between there.
Another thing I should point out with AHIMA. The AAPC’s exams are always going to be offered through a local chapter, usually. They’re always going to be proctored. They may be offered through a local community college, may be offered through a local chapter, those types of things. AHIMA’s you’re going to go to a testing center, like, Pearson Education Center; that sort of thing. The AAPC, if you need to cancel, you can reschedule your exam, you can cancel your exam, you’re going to pay a minimal fee. With AHIMA, if you have to change something, you forfeit your entire registration cost. If you got your name wrong – yes, people get their name wrong sometimes – you forfeit that entire registration.
Laureen: I didn’t know that part.
Chandra: I actually had a colleague who was married and her last name was hyphenated but she didn’t formally change it. When she signed up for the exam, she used her hyphenated last name. Well, when you go to register – and she gave them her driver’s license, it didn’t match. They won’t allow her to test and she lost her entire cost of her exam because she didn’t follow the directions. It has to be perfect.
Laureen: Oh, wow.
Chandra: The CIC includes inpatient coding and a little bit of outpatient methodology. I think there are five questions, something like that, it’s very minimal. The AHIMA side is going to test you on both inpatient and outpatient. It’s a full facility credential, instead of just inpatient. The books for the AAPC side, you take both of your I-10 books; your ICD-10-CM for diagnosis, PCS for procedure. AHIMA, you need both of those plus your CPT book. Again, we’re adding a whole another piece in there that we wouldn’t have to have.
Laureen: What about HCPCS?
Chandra: No HCPCS books for either.
Laureen: OK.
Chandra: AHIMA actually has a list on their website much like the AAPC does, only AHIMA has a downloadable PDF to tell you which books and publishers are allowed, and HCPCS is not one of the manuals that they include for the CCS.
Laureen: I was really surprised the last time I took the CCS back in the day and it was the only one that I didn’t pass and I had to take twice. It was the last one I took which says a lot because I knew coding but I wasn’t fast, which comes with experience, because I was teaching it, I did it in my rehab practice but I didn’t do stacks of coding, and that’s what it requires to get really proficient and fast. They’ll tell you on the AHIMA website that the CCS is really a master-level credential, not an entry level. It’s designed to tell the world, “this person has been doing this for several years and they’re at this very high level.”
Nowadays, what’s happening is, people see job want ads for CCS, and they’re like, “Oh! I’ll go get that, and I’ll go study and take the exam and then I can go get those jobs.” That really wasn’t how it was designed. Now, the CPC and the CCS-P and the CCA (which is like the junior CCS credential, if you will), those are all entry level. They’re still hard, very hard, very challenging, it proves you know coding, but there isn’t this expectation of experience with it. That’s just something to understand, and that’s why the pass rate, the last I heard for the AHIMA CCS was like 40% only, because so many people sit for it that really shouldn’t be sitting for it. They’re just not ready.
So, that one took me twice, and then unfortunately I let it lapse, so my mom got sick and when I went to retake it, it was right on the heels of – I can’t remember, some major thing happened. I just remember being a really bad day but I didn’t want to give up the money, like Chandra said, you forfeit it. I said, “Oh, I’ll just go do a Hail Mary and see.” There was lots of CPT on it from when I remembered before. So, a lot of people think of the CCS as an inpatient credential and it’s really not. It’s like an everything credential; it’s inpatient, outpatient.
Chandra: And a lot of people may be looking at like this basic information I put together, and if you already have your CCS and you’ve got it prior to the transition to ICD-10, these numbers were a little different because I took mine right before the transition to ICD-10, because even though I was teaching ICD-10, I wanted to get it done in I-9 because I had more of those codes memorized. It was still right around 97 multiple choice, but there were also like 12 multiple select and there were 10 medical scenarios (5 inpatient and 5 outpatient), and they’ve changed very much the way that they’ve structured that portion of the exam now that we’re in ICD-10. I’m sure they probably cut the scenarios back thinking it takes a little longer to code it in ICD-10 especially with PCS, but it is a little different than it’s been in the years past.
Laureen: So, what do you think as far as a first credential? Do you think the CIC is a good first credential, or do you think it’s better to still get your CPC than the CIC? I know what you’re going to say – it depends.
Chandra: That’s my favorite answer, you know this. If the person is wanting to work in the facility side of things, I don’t see a problem with getting the CIC. Just know you’re probably not going to have the CPT experience, especially if you take a course that is just for the CIC, you’re not going to have the CPT skills because the CIC only includes ICD-10-CM and ICD-10-PCS, which is what you would use on the inpatient facility side of things. But many inpatient facility coders also wind up doing some portion of outpatient facility coding or the COC stuff, in which you’ve got to know the CPT side of things.
Laureen: Yeah. We should talk about that a little bit because that confused me initially. The AAPC always had the CPC, and then the CPC-H, which changed its name to COC (Certified Outpatient Coder). It was very confusing because a lot of people thought “H” meant inpatient like “hospital.” And it did, it meant “hospital” but hospital out…
Chandra: It only meant hospital outpatient.
Laureen: Right. Like I was one of the ones, I studied like PCS and went, “I’m ready for my inpatient stuff,” and I’m going through the exam, like, where’s the PCS stuff? It’s all CPT.
Chandra: Not there.
Laureen: It wasn’t there. So, to me, the COC is like a glorified CPC exam with a little bit of outpatient reimbursement questions. Because really, the coding is the same; so that’s a nice stair step if you want to get multiple credentials, CPC then COC. Now, they have the CIC, which I love because like Chandra said when you put them together, the COC and the CIC, I feel those equal the level of the CCS exam that you can get as an entry level and then make that CCS. If you want to be in both organizations, which I don’t think as a bad thing, then you can aspire to that, but don’t make it your first credential. That’s just really reaching for the stars too quick, and you’ll spend a lot of money, having to do retakes. It’s discouraging, I would think, to start with that.
Chandra: I would agree.
AAPC CIC vs. AHIMA CCS Exams: Competencies
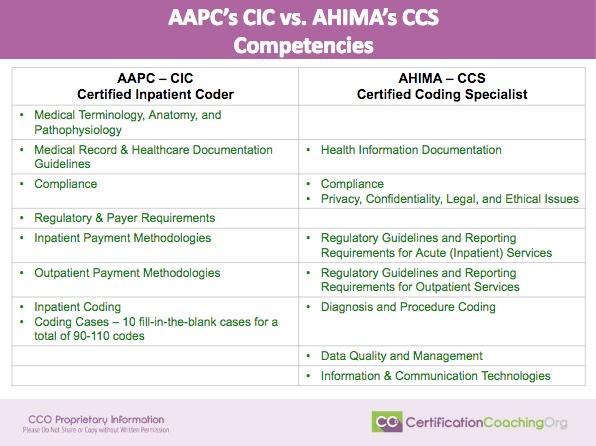
The next slide that I have is just going back through the competencies, which we’ve already kind of discussed, so I won’t waste a bunch of time there. But I did put together a graphic on the next page that I thought was kind of interesting. I wanted a way to show these two side-by-side. Basically, what I did was I took this slide of the competencies, and if you figure each one of these has their own color; medical terminology, anatomy and patho, that was one. CCS don’t have any of it, has its own bucket on there. I won’t say it won’t affect your exam, because it will. It’s just not a discrete domain that they worry about. I kind of lumped compliance and privacy and confidentiality issues together. Regulatory & payer requirements, after is inpatient, outpatient. All the diagnosis and procedure coding, there’s two areas on the AAPC, only one on AHIMA. Then, there are these two areas that AHIMA test on that AAPC does not.
AAPC CIC vs. AHIMA CCS Exams: Competencies Compared
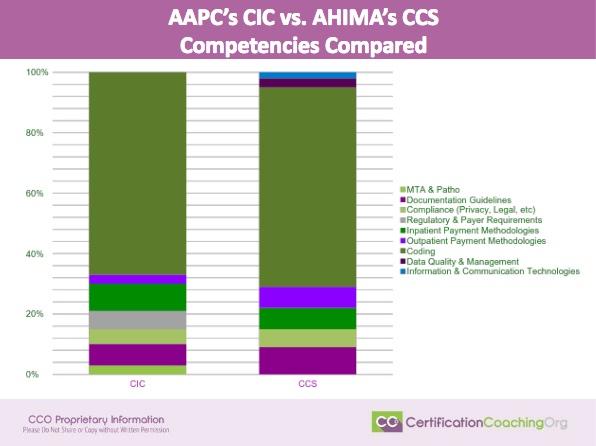
The next slide just shows you stacked up against one another, the largest area on both exams is still the coding. It’s about 66% on the CCS, it’s 67% on the CIC, if you lump the coding together. But then, that’s when you see, OK there are two little bars here that are on AHIMA’s that are not on AAPC’s. There’s a bar down here on AAPC’s that’s not on AHIMA’s, that’s not med term and anatomy piece.
It was a good visual for me to go, “Oh! There’s a lot less outpatient on this one than there is over here. There’s a little more inpatient methodology than there is over here.” “Oh! They test me on regulatory and payer requirements, but they don’t call it that over here.” Just so I can see, again visual.
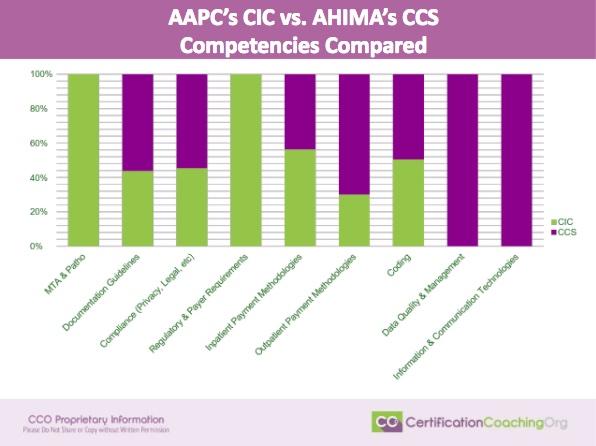
The last graphic that I have kind of does the same thing, but instead of by credential, it’s by domain. So, these are all the different areas and this shows you, if it’s in green, it’s the CIC exam. If it’s in purple, it’s the CCS. You’ll notice, medical term, anatomy and patho, that whole thing is just the CIC; it’s not on the CCS at all. The documentation guidelines, well, there’s more of it on the CCS than there is on the CIC. Those types of things.
Laureen: It’s not to say you don’t need the medical terminology and patho, it’s baked in. You just have separate individual questions.
Chandra: It’s not pulled out separately, right.
Laureen: Like, “Hey! I’m a medical terminology question.” [Laughs] But, if it’s built into the scenarios you’re reading; so you still need to study it.
This segment “Comparing AAPC CIC and AHIMA CCS Exams” originally aired on Live with Laureen #013 on January 5th, 2017.
I have a question. I have already attained my CCS. Do you recommend that I also attain the CIC and COC?
thanks in advance,
lisa
The CIC + COC equals the CCS in my opinion. I’d go for a specialty credential that shows you have additional skills vs the same ones. Like risk adjustment (CRC) or auditing (CPMA) or compliance (CPCO). –Laureen
With the RHIT being phased out and a lot of employers requiring a CPC or CCS, would you recommend a RHIT to get a CPC or CCS, or go for Specialty certification instead?
Hi, I have a question to ask. I have the CPC and want to learn inpatient coding. Which would be better? A CCS or COC and CIC together. Would having COC and CIC give an advantage over CCS? If possible, I would prefer to stick with AAPC because I liked their format for the CPC and I did very well with it!!
Laureen’s earlier comment answers this pretty well. In addition, we recommend looking at local jobs to see what inpatient credentials are popular in your area. It varies quite a bit from region to region and you want to make sure you have the one that is popular locally.
What are your opinions on starting with the CCA instead of COC+CIC, if my goal is still the CCS in the future after a few years of working?
My local job market is pretty open to CCAs at the entry level.
The local job market dictates demand more than anything else. With the CCA, you cannot remove the “A” in the CCA. The CCS is a better choice as it’s the next step up. But again, if local jobs are looking for the CCA, than that’s your best chance of making yourself marketable.