M
Mayenne Perpetua
Guest
Visit [CCO] Certification Coaching Organization LLC for more articles about [CCO] Certification Coaching Organization LLC - Medical Certifications - Learn It - Get Certified - Stay Certified.
Q: “I would like for you to go over TCM leveling for the physician’s office. My understanding is that it is based on the medical decision making only, but I would like to learn more about it. Could you possibly discuss this in the next monthly Q&A webinar?”
A: Tonight that’s what I will be addressing. Before I go into Medical Decision Making, I will talk about some of the requirements that’s required for the TCM services. The first one is: “The services are required during the beneficiary’s transition to the community setting following particular kinds of discharges.” That means that when the patient is discharged, say, from the hospital, community setting can be anything from a nursing home, a rest home, the patient’s residence (his actual home), but it’s the discharge to wherever that patient is living.
“The health care professional accepts care of the beneficiary post-discharge from the facility setting without a gap.” They go right into it. TCM starts the day of discharge.
“The health care professional takes responsibility for the beneficiary’s care.”
“The beneficiary has medical and/or psychological problems that require moderate or high complexity medical decision making.”
VIDEO: Transitional Care Management (TCM) – MDM Leveling
In order to qualify for TCM coding, you have to have either moderate or high complexity.
The 30-day TCM period begins on the date the beneficiary is discharged from the inpatient hospital setting and will continue for the next 29 days. So, that if January 1st they’re discharged from the hospital, that’s day 1; and on January 30th, 29 days after that, that is the date of service that you would use to bill or code the transitional care management service.
Face-to-Face visit – You must furnish one face-to- face visit within certain timeframes as described by the following two CPT codes: CPT code 99495 is the TCM with moderate medical decision complexity. That means that face-t- face visit within 14 days of discharge. The 99496 is the high medical decision complexity. That has to be done within 7 days of discharge. Keep in mind that the face-to- face visit is part of the TCM service and you should not report it separately.
It really is important that once you determine that you continue to call that patient until you see them or to contact them on the telephone depending on the situation but it has to be within that timeframe.
Medical Decision Making – Refers to the complexity of establishing a diagnosis and/or selecting a management option, which is determined by considering the following factors:
The chart below depicts the elements for each level of medical decision making. Note that to qualify for a given type of medical decision making, two of the three elements must either be met or exceeded. The next page will show the actual chart and you will see this in the front of the CPT manual as well, but you will be focusing on the last two – the moderate complexity with the multiple diagnoses and/or management options, moderate amount and/or complexity of data to be reviewed, and also moderate risk of significant complications, morbidity, and/or mortality. The high complexity which is the other option, everything is extensive and high risk.
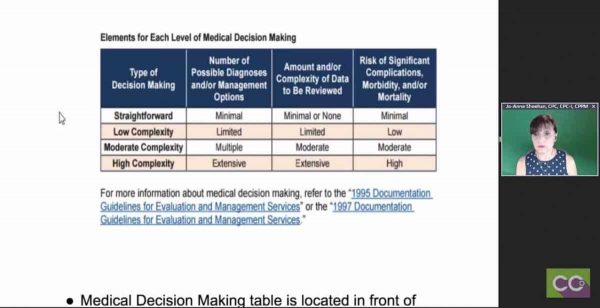
Those are the bottom two that you would focus on if you were going to code for TCM upon a discharge. I will have a link where you could actually click on to the ’95 and ’97 documentation guidelines. But the medical decision making table is located in the front of your CPT manual. And as we learned from Laureen from her E/M presentation, that when you are working with medical decision making, two of three elements must either be met or exceeded and you always drop the lowest.
If we go to the CCO.us there is an Understanding E/M Coding Step-by- Step Guide and the medical decision making explanation is incorporated into this and that will also help you to determine what level of medical decision making you would need.
Medication Reconciliation and Management – Keep in mind that the medication reconciliation and management must also be furnished in no later than the date you furnish the face-to- face visit, and that’s very important.
Billing TCM Services – When we’re billing:
1) Only one health care professional may report TCM services.
2) Report services once per beneficiary during the TCM period.
3) The same health care professional may discharge the beneficiary from the hospital, report hospital or observation discharge services, and bill TCM services. However, the required face-to- face visit may not take place on the same day you report discharge day management services. Because technically, a discharge is a 99238 or 99239, which is a discharge, it’s an E/M code so you’re not allowed to code for that, it’s all bundled in.
4) You can report a reasonable and necessary evaluation and management (E/M) services (other than the required face-to- face visit) to manage the beneficiary’s clinical issues separately. I have seen multiple times primary care physicians when they’re managing a patient that is involved with the TCM, that they do incorporate the face-to- face or the communication between the patient or a guardian in their TCM, but sometimes the patient will go in on the exact day that they’re billing for the TCM, on that 30th day and they can actually bill for a visit. So, if a patient came in for a different problem that is not face-to- face that’s built into the TCM code, you can bill an E/M with the TCM and add a modifier to the 99213 or 14 or whatever the E/M service is, but it is not the E/M that’s incorporated into the TCM code.
5) You may not bill TCM services and services that are within a post-operative global period, like a 90-day global period, so keep that in mind. Also, you cannot report the HCPCS codes G0181 and G0182, the Home Health Care, Care Plan Oversight, and you cannot bill the end-stage renal disease services, also the Chronic Care Management (CCM) services. And so, all of these cannot be billed in addition to the TCM.
Frequently Asked Questions about Billing the Medicare Physician Fee Schedule for Transitional Care Management Services:
 This is a link that you’ll be able to have a lot of your questions answered, any of your questions that you might have in regards to TCM that I haven’t covered tonight. That is one portion that you can review and some of it has already touched on what I’ve talked about, but there are other things, like if a patient is readmitted or things like that. Very specific. There’s a lot to it, it’s not just medical decision making, but this one form.
This is a link that you’ll be able to have a lot of your questions answered, any of your questions that you might have in regards to TCM that I haven’t covered tonight. That is one portion that you can review and some of it has already touched on what I’ve talked about, but there are other things, like if a patient is readmitted or things like that. Very specific. There’s a lot to it, it’s not just medical decision making, but this one form.
My other link that I have is, this is wonderful. This is where I actually got all my information even though I knew it, I took it the way Medicare Learning Network presented it and it’s phenomenal. That’s eight pages that you can print out and it gives you everything. Like I said, I just touched on a couple of things but there is a lot more information built into this and it will help you. I just touched more on the medical decision making and some of the codes that you can build into it, but this will help you quite a bit and there are a lot of links there in the ’95 and ’97 guidelines for coding, so that should help you. Basically that’s it. You just want to make sure that if you are coding for TCM that it is a moderate or high complexity medical decision making. That’s very important.
Laureen: Thanks Jo-Anne.
Jo-Anne: You’re welcome.
Laureen: Just to let the people know I did put the links of those last two items in the chat if you want to grab them because that’s an awful long one to try and have right now. And someone was asking in the chat about getting the answer sheets. The answer sheets are available to our CCO Club members, which is $20 a month. You get the full replay of this whole webinar, you get the CEUs built into it instead of having to pay the $5. You get a full transcript about a week later. It’s a lot of goodies that come with it. But the regular handouts, the slide deck handouts are in the GoToWebinar panel window, you can find it there.
Related Transitional Care Management (TCM) Services Posts:
The post Transitional Care Management (TCM) Services – MDM Leveling appeared first on [CCO] Certification Coaching Organization LLC.
Continue reading...
Q: “I would like for you to go over TCM leveling for the physician’s office. My understanding is that it is based on the medical decision making only, but I would like to learn more about it. Could you possibly discuss this in the next monthly Q&A webinar?”
A: Tonight that’s what I will be addressing. Before I go into Medical Decision Making, I will talk about some of the requirements that’s required for the TCM services. The first one is: “The services are required during the beneficiary’s transition to the community setting following particular kinds of discharges.” That means that when the patient is discharged, say, from the hospital, community setting can be anything from a nursing home, a rest home, the patient’s residence (his actual home), but it’s the discharge to wherever that patient is living.
“The health care professional accepts care of the beneficiary post-discharge from the facility setting without a gap.” They go right into it. TCM starts the day of discharge.
“The health care professional takes responsibility for the beneficiary’s care.”
“The beneficiary has medical and/or psychological problems that require moderate or high complexity medical decision making.”
VIDEO: Transitional Care Management (TCM) – MDM Leveling
In order to qualify for TCM coding, you have to have either moderate or high complexity.
The 30-day TCM period begins on the date the beneficiary is discharged from the inpatient hospital setting and will continue for the next 29 days. So, that if January 1st they’re discharged from the hospital, that’s day 1; and on January 30th, 29 days after that, that is the date of service that you would use to bill or code the transitional care management service.
Face-to-Face visit – You must furnish one face-to- face visit within certain timeframes as described by the following two CPT codes: CPT code 99495 is the TCM with moderate medical decision complexity. That means that face-t- face visit within 14 days of discharge. The 99496 is the high medical decision complexity. That has to be done within 7 days of discharge. Keep in mind that the face-to- face visit is part of the TCM service and you should not report it separately.
It really is important that once you determine that you continue to call that patient until you see them or to contact them on the telephone depending on the situation but it has to be within that timeframe.
Medical Decision Making – Refers to the complexity of establishing a diagnosis and/or selecting a management option, which is determined by considering the following factors:
- 1) The number of possible diagnoses and/or the number of management options that must be considered.
- 2) The amount and/or complexity of medical records, diagnostic tests, and/or other information that must be obtained, reviewed, and analyzed.
- 3) The risk of significant complications, morbidity, and/or mortality as well as comorbidities associated with the patient’s presenting problem(s), the diagnostic procedure(s), and/or the possible management options. There are lots to consider when you are coding for the TCM.
The chart below depicts the elements for each level of medical decision making. Note that to qualify for a given type of medical decision making, two of the three elements must either be met or exceeded. The next page will show the actual chart and you will see this in the front of the CPT manual as well, but you will be focusing on the last two – the moderate complexity with the multiple diagnoses and/or management options, moderate amount and/or complexity of data to be reviewed, and also moderate risk of significant complications, morbidity, and/or mortality. The high complexity which is the other option, everything is extensive and high risk.
Those are the bottom two that you would focus on if you were going to code for TCM upon a discharge. I will have a link where you could actually click on to the ’95 and ’97 documentation guidelines. But the medical decision making table is located in the front of your CPT manual. And as we learned from Laureen from her E/M presentation, that when you are working with medical decision making, two of three elements must either be met or exceeded and you always drop the lowest.
If we go to the CCO.us there is an Understanding E/M Coding Step-by- Step Guide and the medical decision making explanation is incorporated into this and that will also help you to determine what level of medical decision making you would need.
Medication Reconciliation and Management – Keep in mind that the medication reconciliation and management must also be furnished in no later than the date you furnish the face-to- face visit, and that’s very important.
Billing TCM Services – When we’re billing:
1) Only one health care professional may report TCM services.
2) Report services once per beneficiary during the TCM period.
3) The same health care professional may discharge the beneficiary from the hospital, report hospital or observation discharge services, and bill TCM services. However, the required face-to- face visit may not take place on the same day you report discharge day management services. Because technically, a discharge is a 99238 or 99239, which is a discharge, it’s an E/M code so you’re not allowed to code for that, it’s all bundled in.
4) You can report a reasonable and necessary evaluation and management (E/M) services (other than the required face-to- face visit) to manage the beneficiary’s clinical issues separately. I have seen multiple times primary care physicians when they’re managing a patient that is involved with the TCM, that they do incorporate the face-to- face or the communication between the patient or a guardian in their TCM, but sometimes the patient will go in on the exact day that they’re billing for the TCM, on that 30th day and they can actually bill for a visit. So, if a patient came in for a different problem that is not face-to- face that’s built into the TCM code, you can bill an E/M with the TCM and add a modifier to the 99213 or 14 or whatever the E/M service is, but it is not the E/M that’s incorporated into the TCM code.
5) You may not bill TCM services and services that are within a post-operative global period, like a 90-day global period, so keep that in mind. Also, you cannot report the HCPCS codes G0181 and G0182, the Home Health Care, Care Plan Oversight, and you cannot bill the end-stage renal disease services, also the Chronic Care Management (CCM) services. And so, all of these cannot be billed in addition to the TCM.
Frequently Asked Questions about Billing the Medicare Physician Fee Schedule for Transitional Care Management Services:
My other link that I have is, this is wonderful. This is where I actually got all my information even though I knew it, I took it the way Medicare Learning Network presented it and it’s phenomenal. That’s eight pages that you can print out and it gives you everything. Like I said, I just touched on a couple of things but there is a lot more information built into this and it will help you. I just touched more on the medical decision making and some of the codes that you can build into it, but this will help you quite a bit and there are a lot of links there in the ’95 and ’97 guidelines for coding, so that should help you. Basically that’s it. You just want to make sure that if you are coding for TCM that it is a moderate or high complexity medical decision making. That’s very important.
Laureen: Thanks Jo-Anne.
Jo-Anne: You’re welcome.
Laureen: Just to let the people know I did put the links of those last two items in the chat if you want to grab them because that’s an awful long one to try and have right now. And someone was asking in the chat about getting the answer sheets. The answer sheets are available to our CCO Club members, which is $20 a month. You get the full replay of this whole webinar, you get the CEUs built into it instead of having to pay the $5. You get a full transcript about a week later. It’s a lot of goodies that come with it. But the regular handouts, the slide deck handouts are in the GoToWebinar panel window, you can find it there.
Related Transitional Care Management (TCM) Services Posts:
- Copayments, Coinsurance and Deductibles and Payer Payments
- Breast Cancer Specific Details Now Required | Medical Coding Guidelines
- Coding Hypertension Controlled vs. Uncontrolled
The post Transitional Care Management (TCM) Services – MDM Leveling appeared first on [CCO] Certification Coaching Organization LLC.
Continue reading...