
How to Pass Your CPC Certification Exam (Video Transcript)
Hello everyone!! We’re really glad that you’re here tonight. We have got something to talk about that really wears on everybody: getting ready to take your certification exam and how do we pass that exam. It is much more than just being a really savvy coder and we’re going to talk about that tonight as well as several other things, tips, we’re going to give you examples and we’re just going to walk you through the testing process, so you know what to expect.
Let’s get started. Thanks for joining us. If you have any questions during the presentation, feel free to pop them up and we’ll go over those maybe during or at the end but we’ll get your questions answered. Grab yourselves something to drink, I got myself some nice tea with one of my favorite teacups and let’s start with: “How to pass the CPC® Exam.”
Step 1: Take a Course
I have to tell you that even if you are the best coder and maybe you haven’t got certified yet or you’ve done really well in your courses but you go to take the test, that doesn’t mean you’re necessarily going to pass the exam, it’s much more than that like I said before. What does it take to pass that exam? First thing, you really need to take a course and you say, “Ok, well, do I really need a course because I already work with codes, I’m already doing coding. Do I need to take a course?” The great thing to do, to see if you need to actually take a course, is jump out and take a practice exam. We have lots of practice exams at CCO and we have free practice exams as well as paid ones.
That’s what you want to do, you want to take a free practice exam and even if you don’t want to take a entire CPC® practice exam but maybe you want to take an ICD-10 practice exam, we got those and we got a free one for you; so those will be linked at the bottom. You’ll be able to get those at the YouTube video on our YouTube channel. That will tell you that if you can’t pass that practice exam, then you definitely need a course. And don’t worry, you may think, “Ugh, I don’t want to start all over.” You may not have to. Use the course as a refresher.
At CCO and maybe some other places I don’t know, I think we’re pretty generous with ours. We give you several months of access. So even after you have taken a course, passed the exam and you want to keep checking in to keep things fresh, we’ll let you have access to your course for a long time and if you want to keep it longer than that, then that’s fine. But, the key is being able to jump into a medical coding course, refresh your knowledge and it’s all about the guidelines.
Maybe you’re the best coder for your area but you code for a niche market. If you’re doing just orthopedics, that’s not going to help you with the pacemaker replacement question, or maybe you don’t deal with a lot of modifiers and there’s definitely modifiers that they’re going to test you on in the exam. Taking a course is vital, that’s part of the proven process that the CCO has. In fact, we have a big video. It’s not that big but it’s a little bit longer video about the proven process itself, I encourage you to take some time and go look at that if you’re trying to make a decision whether you need to take a full course or what you need to do to set up yourself for success in the career of coding.
Step 2: Refine, Refresh and Review
The next thing is step 2. We call this, “Refine, Refresh, and Review your skills.” Now, this is really getting into the guidelines and that’s what the exam is mostly about, I mean anybody can look up a code. It’s like looking up a phone number in a telephone book, which actually is something that’s a tad bit outdated now that I think about it. I don’t even know if my children could look up a number in the telephone book. Looking up a word in a dictionary, even then with our computers it might be a little outdated.
But we’re going to specifically talk about step 2 tonight. I got some examples and that’s where you know how to look up a code, you know the details but now you need to get really good at your knowledge base so that you can do it more efficiently, quickly and to the highest specificity on the codes because they are going to test you on that.
Step 3: Practice Exams
Third step: practice exams; you need to take as many practice exams as you can get your fingers on and again, there’s several out there. I would encourage you to make sure you go to a reputable source that would be like anything. Don’t be investing a lot of money on practice exams if you aren’t confident on where they’re coming from because… we’ve been told our practice exams are harder than the real CPC® exam and I appreciate that, but our rationales are what put them over the top.
If you have 4 choices, we don’t just explain why “B” is the right answer, we tell you why A, C, and D are the wrong answers and that’s what you’re going to need to look for when you go to take your practice exams. Sometimes they just score you. If you’re going to take an online practice exam, they just give you a score, but they don’t give you any rationale and talk you through why you missed it. But then after that you’re ready to sit for your certification exam, we have videos out there on our YouTube channel about how to set up, how to register for the exam. And of course, you can come into our Club anytime and ask questions like that, so feel free to take advantage of those resources.
Before you test, again the proven process that I mentioned before, I want to really focus on step 2 and one of the things that we have is our Blitz (bubble highlight and annotate technique). We even have what we call a BHAT® cave because it spells B-H-A-T. That allows you to get your CPT® manual ready for testing. We have a lot of positive feedback about after they went ahead and used that BHAT® technique on their CPT® manual that they were able to pass their exam when they weren’t able to do it before and one of the reasons is it makes the codes pop out at you and it’s less likely that you’re going to get confused because quite honestly, you’re sitting there for 6 hours and it is difficult to keep your brain focused and flipping through pages for 6 hours. You kind of zone out and you get in the groove. But, you need something to give you all the advantages that you can and so that BHAT technique does that.
Step 4: Know Your Guidelines
The guidelines, I can’t reiterate it enough. We tell everybody in our course and this is what you need to do as well. The HCPCS®, mind you, that’s just like the CPT® manual, there’s not a lot to talk about the HCPCS® because if you can do CPT®, you can do the HCPCS® manual so set that aside. There are only 5 questions on the HCPCS® in the AAPC’s CPC® exam. Don’t let yourself get nervous about not being confident with that particular code set; if you can do CPT®, you can do HCPCS®.
CPT® and ICD, they have guidelines and you’re being tested on the guidelines. You need to read each of these guidelines at least 3 times. What I tell the students when I talk to them is a good plan of action is when you first get your manual and you take off all the plastic and everything, it’s all shiny and new. You’re all excited about getting started in this new career path and training. You’re going to open that manual up either one, CPT® or ICD. ICD is really thick; it’s twice as big as the CPT® manual. You’re going to look at that and it’s going to be like you’re punched in the gut at first because it is extremely intimidating, there’s just a lot of words in there and a lot of things that you may not even understand. Maybe you’re taking your anatomy and physiology at the same time you’re taking your coding course or medical terminology and anatomy, and even to this day. I’ve literally been in the medical field for over 30 years and I still will look at my manual and think, “I don’t even know what that word is. It’s not a word that’s got a prefix or suffix to it that I can break it down. I don’t even know it, let alone pronounce it.”
Again, do not get intimidated by that. Relish it, enjoy it because this manual in both CPT® and ICD, you’re going to get up close and friendly with for a long time even after you passed the certification exam, you’re going to treasure those manuals, and every year you’re probably going to get new manuals and make notes in them even if you used an encoder. Just like a favorite book that you have dog-eared from using over and over again, that’s what I expect to happen with the guidelines in both the CPT® and the ICD.
Also, when you go through these guidelines the first time, just read through them. And I don’t expect you to read word for word. Peruse them thoroughly, a little light reading is the way I would think of and think, “Oh yes, this interesting”, “Oh, we’re going to talk about the symbols that are in the manual.” And then you’re looking at the guidelines and it’s going through the disease process or the body systems but you’re getting a feel for the layout and both of them are just outlines.
So if you remember in school, if it was in your junior high or high school when you learned how to create outlines, that’s exactly what the guidelines are. They are an outline of how to use the manuals. And then when you’ve gone through that, then you’re ready to take the course and start the course step-by step and each one of the chapters in your course will reference back to those guidelines again and again.
I would encourage you to have a notebook. I always got paper around me, but get yourself a little spiral notebook and whenever you see something you don’t understand, make a note on it and you’re going to be able to build on those notes as you go through your course or as you study for the certification exam. There’s something about tactile learning, just writing things out even if you’re rewriting a sentence or a statement that you see in your guidelines, it will stick in your brain better. I used to have a college roommate and she used to type out all of her notes, she used to write notes in longhand and then she would come home and she would retype all of her notes and I just thought that was nuts. However, her typing them made them stick in her head. You may want to create something like that for yourself but I think just writing out anything you have a question about so that you can go back and reference it or you find the answer and then write that answer to your question or the statement that you found in your book. It’s almost like your journaling along the journey.
The guidelines – so you’ve gone through the course, about halfway through the course if you haven’t already started the BHAT technique, the bubble highlighting annotating, then that’s where you’re going to end up going in and reading those guidelines a second time. And unlike the first time, you are going to dwell down in them; you’re going to really pay attention to the details. It’s going to take you longer to get through them the second time. We’re not perusing anymore, we’re actually looking at the guidelines.
Now, I pulled out some guidelines to highlight to show you how you can do this. When you go through the BHAT® technique for the CPT®, you’ll be making notes. And then we have annotation for the ICD-10 as well to help you with those guidelines and it will make everything pop for you. There you go: guidelines, 3 times, third time before you test. So you’ve already taken your course, you’ve perused through the guidelines to kind of say, “Oh, what have I gotten myself into?”
During your course, you’re really going to delve in, pay attention and make notes for yourself and use the BHAT technique, but then, the last time or the 3rd time that you read them from start to finish, this is really just in a calm way going through them again and making sure that you have that information in your knowledge base and that there’s not something that you think that you need to at the last minute go look up. I encourage you not to overthink things, don’t over-markup your manuals; that’s another thing that that notebook is for. You can scribble and make notes and squiggles and all kinds of things, but when you put that into your CPT® manual or your ICD and you’re putting in the annotations and stuff, you’re going to be very methodical and neat and just make sure that it’s not going to get confusing.
I once had a student that had every highlighter color that was known to man. Her desk was right close to mine and as a student… I had these 3 advanced students. I used to have them sit up closer to me because we would go over stuff where the other students were not in advance and their hours overlapped. She just laid out all these highlighters and then she started highlighting in her manual and her textbook and stuff. It was just a collage of colors and I kept asking her. I said, “That’s really confusing, I don’t know that I would go as far as you are,” and she was like, “no, this is what I have to do to study, this is the way I learn.” I was like, “Okay, that works for you.” So I encourage you not to go overboard but be very concise and precise about what you put in your manual so when you do sit down and test, it’s not confusing to you.
CPC® Tips Straight from the AAPC
Let’s talk about tips for the CPC® exam straight from the AAPC. They are the ones that write the exam and therefore, they’re the ones you want to get the tips from. We have tips that I’ve been telling you like the ones that I just told you on the previous live. We’ll add stuff to it but let’s talk about what the experts, the ones that wrote the exam, tell you to do. We’re going to go over these and I’m going to give you some more highlights and personal thoughts as we go a couple slides through these tips.
These are straight from the AAPC website; you don’t even have to be a member. You don’t have to log-in to see these… and some of these are great testing tips if you’re just taking classes, I would encourage you to use them. It’s all about the guidelines, you can ask anybody that’s taken the test and they’ll say, “Yeah, it’s about the guidelines.”
When you look at a test question, you almost have to ask yourself, “What do they want to know that I know?” It’s not necessarily about looking the codes up because it’s a multiple choice exam. If it was about you trying to find the code in the manual, it wouldn’t be multiple-choice. You have to be able to determine with those codes which is the highest specificity and the best answer, that’s not always easy to do.
Next, get your materials organized. That’s where the BHAT® technique comes in and you make sure that you have your notes in your manual to test. You can’t write test questions and stuff like that but you can make little annotations about what a specific word means, hypertension is abbreviated HTN. You can put things like that and I would encourage you to get savvy with abbreviations for diseases because they do use those a lot and you should be at that level before you test, that you know them and if you’re not, then you need to take a medical terminology course.
Even if it’s been a while, say, “I took that in college but it’s been 10 years.” I would still encourage you to do this. We have a fabulous MTA course (medical terminology and anatomy) . We’ll put a link in that for you on our YouTube channel so that you’ll know if you think you need that. It might just be a good refresher for you.
Getting organized, don’t overdo your notes and just pick maybe two color highlighters, no more. I honestly use one because I use underlining and I use one highlighter and I use yellow because it pops the most for me. You might say, “I like to use two.” Well you could, but mess with that in your notes first and give yourself an idea of how you want to set it up. For our CPT® manual, we just have you use a yellow highlighter and you’re bubbling around groupings and you’re underlining keywords. Make it simple on yourself, figure out the way you want to do it and stick with that; don’t overthink it.
Sequencing matters – absolutely, you’re tested frequently in sequencing of codes. In fact, when you look at the codes in the multiple choice, sometimes just the sequence of the codes can tell you how to rule out certain choices just like that and we have absolutely education on that and we do a lot of practice of that with our student webinars and our club webinars, and past videos. We have YouTube videos going back almost 10 years. If you want to go back and look at those, I would encourage you to still do that when you look at our channel because maybe some of the codes have changed, not a whole lot but concepts are still the same so if you go back and look at 5, 7, 9 years ago and you’ll say, “I don’t know if I want to watch that video.” The codes may be a little bit different like M18.3 now has additional characters for CKD but the concept of how you stage CKD and how it relates to diabetes or it relates to hypertension. That concept, that stuff is all still the same.
That being said, sequencing, what do you need to know about sequencing? When you look at a code and you are trying to figure out if that is the right code, there are additional notes in your manual that tells you how to sequence. It’s called, “code first” and there is “in addition.” If you see the term, “code first” that means it’s telling you, “Hey you need to code this first before you use the code you’re looking at. If you see “in addition” that means there is another code that you need that will give more specificity.
The example that they’re using here and those are very old codes but again, this came from the AAPC website and we have no control over them updating this information. But, what you’re seeing here is some ICD-9 codes. If you have a person that has a UTI, they come in for the UTI. They get a diagnosis of a UTI. Well, in a UTI there’s an organism or a bacteria and based on what that is tells what type of antibiotic you use. You may have heard them say when you go in with the UTI, “Hey, we send this off for culture and if we need to change your antibiotic based on what the culture says when it comes back, we’ll give you a call. Otherwise just keep using your antibiotic that we give you, it’s broad-spectrum, it’s supposed to take over a wide variety of types of infections that you could have and make sure you finish your antibiotics.”
Well if you get a call, that means that whatever showed up in the culture isn’t maybe the best treated with the antibiotic they gave you. There may be scenarios where… I can’t take Bactrim. Any of the sulfa drugs I can’t take and I can’t take penicillin so that narrows the scope of what I can take for UTIs or other things. Some of it is the preference of the doctor, what they like to prescribe.
That being said, when you have your UTI, that’s your diagnosis but what’s the organism? Well if it’s E. coli, then there are specific medications that work really well with E. coli and E. coli is actually one of the most common that you get. But maybe it’s something else, maybe it’s staph, or etc. but they’re actually listed in the A codes of your manual so it will tell you, “use in addition the code to identify the organism.” And that would be E. coli so use the code for the diagnosis UTI. And then it says, “in addition, use the code to identify the organism.” That means it’s sequenced second.
No brainer, you don’t have to think it through, it’s right there in your manual so don’t sweat it. It’ll tell you, “Hey, this gets coded before this code.” Then another area that you need to be really careful with sequencing is OB codes (obstetric codes). Whenever you see a code that has “O” in front of it, the letter O, definitely take a pause. Pay attention because there are very unique guidelines and scenarios that are applicable to those codes and you’ll learn that in your course.
Parenthetical notes give valuable information – absolutely they do. The parenthetical notes are everything that’s in the parentheses is what they’re called. I always call them brackets but brackets are actually the ones that look like a square cut in half.
Parenthetical notes, anything that’s in parenthetical means you need to stop and read that, it’s applicable to this code. The easiest one to remember and to see is to go look up the code I10 for hypertension. In the past, they used some ICD-9 codes. In the past we had multiple hypertension codes for ICD-9 but then when ICD-10 came around, they used one code (I10) which was easy to remember. In parentheticals they add all the other types of hypertension that you could have: essential, benign, malignant, all these sort of stuff. And they said, “Hey, I10 covers all of those.” That’s in a parenthetical note.
You don’t have to go look anywhere else if the patient has essential hypertension and if it’s not in the parenthetical, then you know it isn’t applicable to I10. Scenarios like that might be a person that has white coat hypertension, have you ever heard of that? It’s a real thing. The patient doesn’t normally have hypertension but every time that a doctor walks in their heart starts to rise and that’s why they call it white coat hypertension.
There’s actually a code for that and it’s not I10 because the patient doesn’t have hypertension, they have another type of heart arrhythmia that isn’t hypertension and so you will not see that in the parentheticals because it’s not one of the hypertensions like primary essential and stuff. So I would encourage you if you’re curious about parentheticals, go get the ICD-10 manual, look at I10, see those parenthetical notes and then just flip through pages. It works for both CPT® and ICD.
If you have a question and you look at choice A and there’s three codes there and you look up the first code and you notice parentheticals somewhere. Maybe it’s underneath the code that says “do not code this with.” And it lists three codes, I guarantee you that your test is being tested on that. ICD will have parentheticals next to the code, the CPT® will have the code and then down below the description it’ll say “do not code with”, or “do not use this modifier.” Things like that. That’s the guidelines and that’s what you’re being tested on.
Know your modifiers – this is a big deal, guys. In your CPT® manual, it’s wonderful, they thought this through, it’s brilliant, they gave you kind of a cheat sheet of the CPT® modifiers right there on the front cover, fabulous. However, there are a few modifiers that get confusing because the descriptions are somewhat the same and that’s where you want to go and look at your appendix A where it gives you a detailed description about the modifier as well as examples of its usage.
Modifier-26 is definitely one that you’ll be tested on, you’ll see it quite a few times in your CPC® exam plus you’re getting tested on the modifiers themselves. So there will be a little section, I think you get like 8-10 questions on modifiers. But you will see modifiers throughout the whole exam and it may help you narrow down to a higher specificity or throw out one option because you know that a modifier is not applicable for that question or when you look at the question or vice versa.
You need a modifier for that, maybe it’s one that doesn’t have laterality built into it and so you need the code for being bilateral because it states plain as day, it’s a bilateral procedure. You looked up the code, “Hey, wait, this doesn’t say it’s a bilateral procedure, I gotta have a modifier. Look at my 4 choices, 2 have bilateral modifiers on them, and 2 don’t.” There you go, you can rule out twp right away, fabulous testing tip. What are they testing you on? Your knowledge of modifiers.
Next, into the guidelines again, what I decided to do was actually look at the guidelines and pull out some examples. To get more information about how to make notes within your modifiers and not overdo it, that’s our BHAT® technique. I would encourage you to definitely look into that. I’ve seen several people already noting in the comment how the BHAT® technique made a difference for them when they tested and so that’s kind of a no-brainer.
But let’s talk about the process. If you want to do this on your own or what it is you need to be able to abstract from the guidelines. One of the guidelines that talks about what the icons are and how to use the manuals and these are guidelines that are at the very top of the guidelines. They always give you a description first like, “this is what this symbol means.” And don’t worry about memorizing those because it’s also written again at the bottom of the pages of your manual, those CPT® and ICD.
None of this stuff you have to have memorized, you just have to be very familiar with it and the more you’re exposed to it, the less you have to think about it. It’s just what I like to call, “A no-brainer, it’s stuck in there.”
Excludes 1 and 2. Pretty critical, you’re going to see that used a lot in testing. Excludes 1, what does it mean? It’s a hard stop and if you don’t know the sign language for stop, you need to learn that. Stop, it means do not ever code this code with the code that you’re looking at. You can’t do them, they don’t go together so here I highlighted, “do not code here.” This code doesn’t get coded and then never, I underlined “never” and then I went on and underlined “An excludes 1 is used when two conditions cannot occur together.”
You were going to see this again and again so instead of having to memorize the whole thing, what are you going to do? What are you going to think about when you see the excludes 1? Don’t code here, hard stop, whatever it takes – no. You can do it this way or you could write hard stop, or you can just write “no,” whatever it takes to say excludes 1, when you see that, don’t put those two codes together.
With an excludes 2 that’s different. It’s a head’s up. Head’s up is different from a hard stop. What it’s doing is it’s saying, “Hey, you’ve got this code that you’re looking at, great code but actually there may be a better code that’s more applicable to your scenario, let’s look at that code too.” So it’s saying, “Hey, either that or this code is not included here.” You’re on the right track but you haven’t quite got it yet. Not included here, I highlighted and then acceptable to use both the codes. If it’s applicable you can use them together when appropriate.
Now, some people forget that, “when appropriate.” Because they think, “Oh no, I can’t code it there.” but actually some of these codes can be put together if applicable and if appropriate. So that means pause, look at it all again, it’s not telling me no, is there a better code or do I need to do more research? That’s the way that you have to look at Excludes 2. These are guidelines and they’re proliferative-ly used throughout the manual.
Let’s look at another guideline. This is the one on HIV, the very first thing you want to know about HIV is you definitely don’t want to code and give somebody HIV if they don’t have HIV. That being said, how would you do that? Well, by using the wrong code. There are codes for testing for HIV being exposed to HIV, an inconclusive test for HIV. Again, they may be appropriate; they are not confirmed case codes. So don’t give somebody HIV and that’s the same way not just with HIV but with all of the diagnoses that you’re looking at.
You don’t give somebody diabetes, you don’t give somebody hypertension and by you putting that code there, you’re giving it to them, you’re saying the doctor diagnosed it because you’re translating. That’s really all we do is that the provider stated that, “Oh by the way that person has hypertension.” No. Or “that patient has HIV.” No they don’t, they just got tested for it.
Under your knowledge base, this is one that they are definitely going to test you on. Guarantee it, you’re going to get at least 1-5 questions on HIV. So you got to know the guidelines and the rules regarding HIV and AIDS. The first thing you need to know is they’re different, HIV is not AIDS. Being HIV positive means you have the HIV virus in your system. It’s asymptomatic that the “A”’ in front of symptoms means you don’t have any symptoms, you’re asymptomatic. The virus is there but you don’t have aids, you’re HIV positive.
When you become symptomatic, then you are not only HIV positive but you’re symptomatic and now you have AIDS which is a different code and you don’t want to give somebody AIDS B20 when they’re actually the Z code for HIV positive. Two separate diagnoses. That being said, only confirm the cases of HIV positive or AIDS are to be put in the patient’s documentation.
How do you sequence with HIV? You’ll notice, see the format of this? It’s just an outline, the guideline is just an outline and I work really well with outlines. I outline my notes all the time just thinking about the process even when I have to do it during a day I’m outlining. I remember when I learned to do outlines in school that I just thought it was really fun. That being said, how do we sequence with HIV? And some of these rules apply to other codes. Again, when you hear the word “sequencing” then they’re going to test you on sequencing.
Selecting the sequencing of an HIV code, what are we going to talk about? Patient admitted for HIV-related condition. What is an HIV related condition? That means the person is symptomatic not asymptomatic. That means they’re not just HIV positive, they have AIDS and so if a patient’s admitted for an HIV related condition, that means they have AIDS. The principal diagnosis should be B20 because that’s AIDS, that’s why they were admitted. The HIV virus followed by additional diagnosis of the related condition that they have. So Kaposi Sarcoma, turns HIV into AIDS, it’s an opportunistic disease and that’s the one they like to use a lot in questions. So the patient’s HIV positive and then they find out that the patient has Kaposi Sarcoma which is a type of cancer and then they’re admitted. What are they admitted for? AIDS and their related condition, so the B20 would go first, the guideline tells you that’s how you sequence it.
Let’s look up the asymptomatic human immunodeficiency virus, this is Z21. This means they’re just HIV positive, they don’t have AIDS. The virus is in their system. If they’re a Z21 then it’s applied for that patient but if you look and you see documentation that states that they’re HIV positive, known HIV, HIV test positive. This is a verbiage that you might see that does not use the term “AIDS”. AIDS is B20, HIV positive is Z21 and also asymptomatic, without symptoms, the “a” means without Z21. If they have AIDS, they’re symptomatic and that’s B20.
Be very careful when using those codes, these are exactly the things that they’re going to test you on and they’re going to use scenarios to see if you’ve got it. That’s all it is, very easy to do.
Practice exams – Before you test, you need to take as many practice exams as you can get your hands on. I know, I already said we’re going to link practice exams and I encourage you to, one, if you’re not sure if you’re ready to test or if you need to take a course, go take a free practice exam and we have a bunch of them for you but when you’re ready to…
You’re getting ready to test, your course is over and now you’re down to the nitty-gritty and you need to start practicing your test taking skills. Your knowledge base, that’s only a part of it, you’ve still got to pass the test and it’s not a board exam because it’s not based on states, board exams are state exams. It’s actually a certification exam, it’s national but think of it like a board exam, a nursing board exam. You can’t go out there and start practicing until you pass the nursing board.
You can’t go out there and start working as a coder until you’ve got that certification, and therefore, you have to be able to pass the test. You may be super savvy, the best coder in the world and you can’t pass the test. I remember a long time ago when Laureen and I first met and she’s been teaching this BHAT® technique since the late 90s, mind you, this is how long ago she came up with the bubble and highlighting technique, and has been actively teaching it.
She said she has a student that was a fabulous coder, was much better than her as a coder but she couldn’t test and she said she took the CPC® exam 5 times. She couldn’t get through the test because she didn’t have good test taking skills at that time and she just didn’t test well. So that’s another reason why Laureen developed these tips and CCO’s BHAT® technique and test taking tips so that it will help people that aren’t good test takers. You know when you see somebody with a plethora of credentials behind your name, you know what that means? They’re good test takers, I’m not negating the fact that they aren’t knowledgeable, they are, but the fact is test taking is easy for them if they can acquire that many credentials.
Take as many practice exams as you can get your hands on and do not schedule your certification exam until you are hitting 85% or better on those practice exams. Then you know you’re going to breeze through the testing process as well as you’re good with your skills and your manuals and your guidelines. 85% are better, maybe 80% but you have to have a 70% or better on the certification exam to pass. There are 150 questions on the CPC® exam, that means that you can miss 40 questions and still pass, that should make you feel really good, that’s almost a whole column that you can miss.
What are those strategy tests? Now we have lots of videos on this but I’m going to highlight some that really have been beneficial and we’ve gotten feedback on and just for personal test taking we know that this works really well.
1 hour per column. It’s in a test grid and you’re going to do one per column, if you’re taking an online test and the AAPC offers that now, that’s different but it’s not really applicable there because they divide the test up into 2 portions. They give you like 2 hours and 15 minutes I think and another 2 hours 15 minutes, it comes out at the same time. You aren’t allowed to take breaks but it’s much faster because you’re literally just clicking versus having to bubble in and making sure you’re in the right place, and etc.
If you’re taking it with a proctor, make sure that you’re able to do 1 hour per column. We can let you print out our practice exams so that you can work on them and then put the information and then you can time yourself and we also… our free practice exams are smaller, so you aren’t sitting there for 6 hours. You can still divide it up. Another thing is the skipping process.
Some of these questions are really lengthy encounters, op reports or visit reports and they’re a page and a half long, don’t let that intimidate you, you don’t have to abstract all of the information out of that to be able to get the right questions. You’re going to look at the codes, see what the codes are telling you by what you know about sequencing and modifiers and the first character of your ICD codes as well as the first character of your CPT® codes will tell you what that code is, because when you’ve worked through your course and everything, you’re going to figure out ways to know what these are like “E” or endocrine codes and “O”- obstetric codes, then “R” are signs and symptom codes. Z codes have their own meaning.
You’re going to be able to say, “OK, this is a page-and-a-half question and that intimidates me, I’m not going to waste my time on that right now, I’m going to skip it,” or “I’m looking and there’s 7 codes for each choice. I’m not ready for that, I’m going to skip it and come back.” Or you can go through and look at it and say, “OK, yeah, I think I know what the answer is.” And “Oh, nope, there’s only 3 codes there but I’m a little confused, I’m spending too much time, skip it and come back.” Very easy to do, and you can make a mark in a text booklet that you’re going to come back to that one later. Because again, you’re on a clock, you’re being timed and you want to get the ones out of the way that you feel comfortable and confident with first.
That being said, when you open up the test booklet and you look at the test grid, actually all the easy stuff is way over at the end of the test. Several people do the test backwards. I am a firm believer of doing the test backwards. Instead of going 1, 2, 3, 4, 5, you do 149, 148, 147 because those questions back there at the end, they’re no brainers, they’re the anatomy and physiology questions. They’re the terminology questions; the HCPCS® is kind of in the middle. You either know it or you don’t know it and you don’t have to look anything up. You don’t have to look up a code so knock those up fast.
I took the CPC® exam twice. The first time I was already coding, I thought, “OK, I’ll just go sit for the exam.” And I didn’t get done in time; I probably could’ve used another 30 minutes and I got through the very end. I had almost one whole column left and you got like 15 minutes left, and so I was just scrambling and filling in the blanks. Well then I looked and I was like, “oh my gosh, these are all the questions I would’ve known just off the top of my head.” And I kicked myself; I missed it by 2 points.
So the next time I went in, I went to the end of the booklet. I know I aced all of those questions and again, you can miss 40 so why waste filling in the blank and guessing on the ones that are super easy. Save those for those ones that are a page and a half or that intimidate you. You get through the whole exam and you hear them say, “Oh, you’ve got 30 minutes left.” I was like, “oh, good!” I went through the whole thing but now there were some here that I didn’t feel confident with, I know where they are in the test booklet because I marked them, I’m going to go through and look at them.
That being said, one more thing, caveat, don’t go changing your answers unless you’re absolutely sure you don’t know what it was because usually in general, your first instinct is correct unless you absolutely know that you did it wrong. Don’t go changing questions; that’s another testing tip for straight across the board all tests. Your gut knows more than you know.
About the CPC® Exam Itself
Let’s talk about the test itself, one of the things that you need to know about is if you’re going to take an online test, there are stipulations that they put you through. One: You have to be in a room with no other electronics. You have to literally have an external camera that you can show the whole room to show that you don’t have your cell phone or other testing devices or a way to look at the exam. If you go to the AAPC website, it’s all spelled out for you on how to do that and what you need to be able to take the online test and the fact that it’s divided up into two.
If you’re doing a proctored exam and we’re back to doing that and honestly I think that’s a great way to test. I know some people are intimidated by it, they’re not ever going to take away the online because that’s like saying, “oh, here’s a lollipop, now we’re going to take your lollipop away.” Know that that is not going to happen.
Visit the Testing Site Beforehand
Locate your testing site before you get started. Say, I’m close to the city capital so the next certification exam I’m going to go to Jefferson City and I want to know where I’m going to test at. It’s all there given to you.
Pay attention to the emails they send you, sometimes your proctors even send you an email with a detailed map and list and helpful tips. Remember, proctored exams, proctors are volunteers and they have to be part of a local chapter, these are people you want to get to know especially if they’re in your area. You should already be a member or you can’t test and you should be making relationships with them ahead of time and going to local chapter events if they’re open in your area or at least reaching out to do that virtually.
I would drive over there and say, “Okay, they’re testing at this particular building.” Not everybody tests at a hospital, people have places that they rent to test some parts of universities, schools and you never know where you’re going to test. One place that I tested in Texas, it was the billing office for one of the members that was an officer and we tested in her office that has a big giant conference room.
Know where you’re going to test because you don’t need to be getting up at 5 o’clock that morning, already being nervous, having your bag and not being able to find the testing center, or there’s just one less worry that you need to add to yourself. Now with Google Maps and everything you can even show a picture, an outside image of the area that you’re going to test. There are also signs usually posted up, they are signs to say, “AAPC tests here” so you’re going to want to look for those signs.
Most people test on Saturdays. If you test on a Saturday, that means that if it’s a hospital or a clinic system or something like that, the offices are usually not open. There’s not going to be a lot of people walking around that can tell you where you’re going to test at, plus it’s quieter so it’s a good thing.
The Day of the Exam
Arrive early. If they tell you that you’re going to be testing at 8 o’clock then you need to be there before 7:30 because that gives you time to make sure you’ve got a good parking space, then you’ve gone to the bathroom, that you have plenty to drink, that you got a tissue and all of your tissue is together. It gives you a little bit of time to be calm before the storm; so arrive early.
If you think you’re going to be late, you need to call the proctor and they’ll have given you a number. So you will call and say, “Hey, I am at McDonalds. I know I’m very close but I pulled over because I realized that there was more traffic than I expected. I think I’m not going to get there at 8 o’clock on the dot.” And they’ll say, “OK, that’s alright, if we know that. I know where you’re at, you’re probably only going to be about 5 minutes late, we’ll wait for you.” Or if you say, “I was on my way, I had a flat tire and I can’t change it on my own, there’s no way I’m going to make it in time.” Then they would say, “Okay.”
Then they know not to wait for you and make everybody else that’s testing wait, so keep that communication open and arrive early, in that way you can pick your good seat where you want to sit etc. Set up your area, bring up your stuff, and usually have a bag. You need to turn in your cell phone, that’s common practice now or if you have an iPhone-watch thing.
And then, what you’re going to do is turn your phone off or you can give it to them or just leave it in your car, say, “I left my phone in my car.” There’s no reason you’re going to need it. I would advise you to have a wrist watch with – I don’t know if you need a minute hand but have a wrist watch, and if you don’t want to look at it, you can at least have it sitting there. You can’t have electronics around you, or anything that could take a picture.
You want to make sure that you have a drink or more than one drink, whether you have a water bottle, be careful about noisy water bottles, most people bring those classes with a straw in it. You want to make sure that you have plenty of whatever you need to drink. Also, some snacks. We’ve done lots of videos on suggestions; we’ve had people talk to us about their suggestions. They say don’t get anything too crunchy because if you get something crunchy, then you could be disturbing other people.
I need to chew; I need to chew on things when I take tests. So either get yourself some gum or look at all the stuff on the other side. Earplugs, if noises bother you, you can get a big giant bag of earplugs then you’re on your own, you can hear yourself breathing. Have your drinks, your snacks, gum or… I have to have protein and I have to have carbohydrates too so I make sure that I’ve got it all even up. Open everything up so you’re not crinkling through the middle of the thing. I get potato chips and I will open up the bag ahead of time and I will have them melt in my mouth because I want the salt.
Bring the Right Tools and Clothes to the CPC® Exam
Make sure you have pencils, the right type of pencils. I would stay away from the little push pencils, you need #2 pencils I think they are. A lot of times in the past, the AAPC used to give the proctors a package of pencils but they don’t do that anymore. So everything that’s provided to you is from that AAPC chapter. Whether they’re pencil snacks. The last place I did a test, they had goodie bags for everybody with a little piece of chocolates, some chewing gum, a little magnet thing and some pencils and an eraser. It was just a really nice little bag, but not everybody does that.
Get comfortable; make sure that you’re not going to be too hot or too cold. I always make sure I have a sweater, something that you can take off or put on, you never know what the air is going to be like. It’s either going to be too hot or too cold, and if I sit for long periods of time, I get really cold. So I advise you, wear socks, don’t just wear flip-flops. There’s nothing worse than having freezing toes and trying to take a test.
Dress comfortably. I wouldn’t necessarily say go in your baggy sleeping clothes or sweatpants with holes in them or something because you are a professional and these are your peers that are going to be around you and seeing you. However, you don’t want to be wearing a big suit and high heels, etc. You want to be comfortable and that’s what everybody expects you to look like.
Don’t Forget to Network
Network, that’s another to get there early, you can’t really talk to people afterwards because they’re still testing or if you walk out together, but even talking in the halls they might be able to hear you. Make sure you have business cards or a way to get your information to the proctors. Thank them for proctoring, they volunteer. This is more than 6 hours for them, this is a whole Saturday most of the time, out of their lives that they can’t get back so make a point to thank them, pass out your cards, be encouraging, positive. Having that positive mindset is going to be one of the best things that you can do for your testing that day.
If you walk in, “Oh, woe is me; I’m probably not going to pass. I’m a really lousy test taker.” Everybody expects you to be nervous, that’s normal and a lot of people have anxiety. Just by giving somebody some encouraging words when you walk in and say, “I really like your glasses” or “Hey, can I walk in with you? I’m not sure where I’m going and you look like you’re confident, know where you’re going.” Or just get to know them, “I haven’t got to a local chapter, are you from here?” And they’ll, “No, I traveled in and I had to spend the night in a hotel last night just so I can test here.” Things like that, get to know these people, they’re your peers.
Example Cases for the CPC® Exam
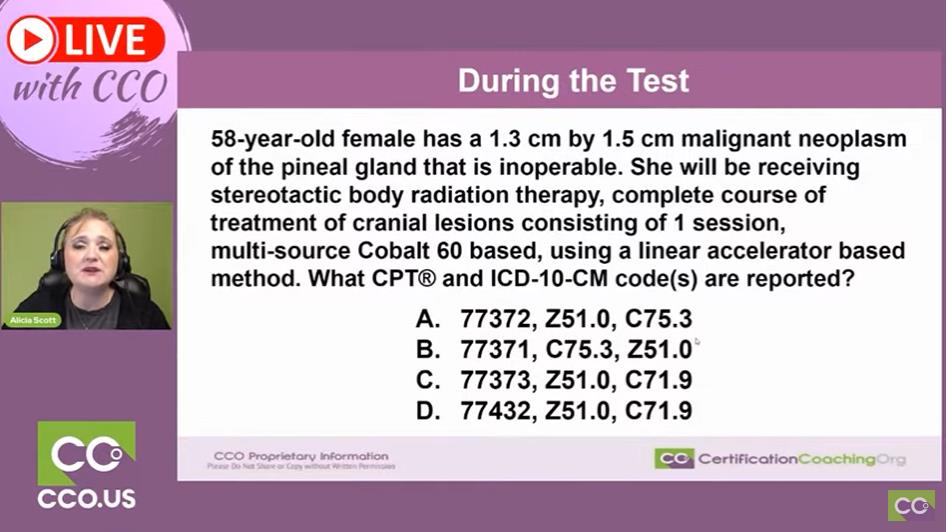
Let’s go through a couple practices here. This is an example of how we do our practice exams. We would do a huge rationale after that. We’re going to abstract from this but this is what a simple question might look like. So you’ve got a 58-year-old female, who has a 1.3 cm by 1.5 malignant neoplasm of the pineal gland that is inoperable. She’ll be receiving stereotactic body radiation therapy, complete course of treatment of cranial lesions consisting of 1 session, multi-source Cobalt 60 based, using a linear accelerator based method.
This is vital. See what they want to know: what CPT® and ICD code(s) are reported? Okay they want to know CPT® and ICD. I’ve read through it but I really didn’t pay attention to anything that I just read because it was just a bunch of… It’s like, “OK, now I’ve got to abstract, what do I need to know?” First thing you do is you look at your choices. You have CPT® and ICD codes.
If you go through your course, you’re going to find out. Are you more comfortable with CPT® or are you more comfortable with ICD? I am definitely a diagnosis person, that’s my passion and if there’s a diagnosis code on a question option then I absolutely am going to gravitate towards that first because they make sense to me and I can rule out really fast. I know that “C” codes are cancer codes, the higher the second character, the closer it is to benign, another type of cancer.
Primary cancers are usually much lower numbers but that’s not way out there. The C75 and C71.9, what jumps out at me with that? The fact that there’s a 9; 9s are usually unspecified. 8s are usually others in ICD, not 100% at the time but as a general rule. It’s a cancer code, the Z71.9 is probably a cancer code that’s unspecified and we have what kind of cancer? Malignant neoplasm of pineal gland, if I were to have to guess instantly, I would not pick “C” or “D” just because of that.
With the other 2, the Z codes are the same all the way around so I’m not even going to pay attention to the Z code. And then there are actually 3 options for the CPT® codes so I definitely need to look them up. However, we’re really lucky because it’s 71, 72, and 73 so they’re going to be right next to each other. That also means the descriptions are going to be close to each other. That being said, that could trick you up really fast.
Just my gut reaction looking at this, probably going to be “A” or “B” and I have no other information for that. Just because I know “C” codes are cancer codes, they’re not that far apart. C75 and C71 but the fact that it’s a 9 makes me think maybe not.
This is how you’re going to mark up your test booklet and you can write all over that thing. I’m going to use my highlighter or pencil whichever you want and I know that it’s a malignant cancer. Because cancer codes are divided up between primary, secondary, benign. I know it’s a primary cancer because no other cancer is written and I know it’s malignant so I know that the C75 is going to be right there C75, C71.
I know the body area, pineal gland, it’s specified and what are they getting? They’re getting radiation and then… now sometimes if they’re going to remove something but they’re not because this is inoperable. Then you’d need to really pay attention to the size of the lesion but this is inoperable, they’re doing radiation so they’re just zapping it. I don’t have to worry about all of those numbers. That can go out; they don’t have to clog up my brain.
They go one session, now that may be pertinent, one session, because sometimes they do multiple sessions and then what are they doing? If I say anything that’s listed in capital Cobalt 60, that’s going to jump out at me, multi-source probably too. This is what my brain would’ve done.
Again, I’m going to look up the ICD codes first. The first one listed is C75.3 so I looked that one up, malignant neoplasm of pineal gland. Yup that’s exactly right. I’m still looking at the other one. C71.9, malignant neoplasm of the brain unspecified, sure enough unspecified. I’m writing a line through those and that means that the Z75.1 is out. “B” and “C” are marked out. Anything that’s 71.9 is out.
Now I need to look at the CPT® codes. 77372, that’s the first one listed so that’s the one I’m going to look up. Sometimes, I go to the lowest number and look it up first to the highest just because I know that it would be sequencing, the codes would be numeric. 77372, radiation treatment delivery stereotactic, SRS, sometimes that would be up there, that wasn’t on there. Complete course of treatment of cranial lesion consisting of one session. You’re right, I’m glad I underlined that. Linear accelerator based, I didn’t even underline that, I underlined the Cobalt 60 so I go back and then look.
Linear accelerator based method. Then I look at 77351 and my eyeball immediately gravitates to “Cobalt 60 based.” I underlined that Cobalt 60 based, so that’s probably the right answer, right? Let’s read it and make sure. Radiation treatment delivery, stereotactic, everything is the same, complete course treatment. Cranial lesion consisting of one session, multi-source, Cobalt 60. So which one is it? Is it 2 or 1?
That tells me that I’ve got to figure it out and if I’m not sure, what are my choices? Well, it says, “linear accelerator based method.” Cobalt it says “multi-source cobalt based.” The fact is that it’s the linear accelerator based is what you need and you don’t even have to look up the Z51 so “A” is the right answer but even if you weren’t sure about those… it’s either “B” or “A,” you’ve already ruled out two so you broke your question down into ruled out 2 right away. Excellent! Easy to do.
What To Do Immediately After Finishing the Test
After the test, what do we do after the test? And mind you that previous, we do that all the time. We break down questions, we set them up like that when we do our CCO Club as well as our student webinars and different webinars that we’ve done on YouTube, make sure you go in and you check those out. There are a lot of changes that happened in E/M and so if you want to make sure that you stay on top of that, you can find out the E/M changes through us as well; so stay tuned to our videos and look at the links to find…
One more thing, when you get ready to test, don’t overdo it by the night before studying and looking things up, that’s just going to cloud your brain. Just go let yourself have a breath and don’t worry about… you either know it or you don’t know it at that time.
So after your test, you’ve tested, everything’s ready to go, what do you need to do? Make sure that everything is filled out on your test grid, that you do not have any missing circles because if it’s not filled out, you don’t get credit for it. And there are 4 choices, so you’ve got 1 out of 4 to be able to get it right and if you’ve ruled out a couple then it’s 50/50 chance that you’re going to get it right. So, look at your test grid but not only do you make sure you have everything circled, make sure your name and all of that other information is on there, that stuff will have been gone through word-for-word ahead of time with your proctor before you guys start the test. Give the test grid back in the booklet to your proctor and do not insert the test grid into the booklet and put the little seals on it. That’s a no-no, you have to do them separate, they actually go into separate envelopes. The proctor has to put all of the test booklets into one envelope and all the test grids into another and then put those all into another envelope and then that’s sent back to the AAPC.
Clean up your area quietly because some people are already testing still, and don’t get intimidated when somebody gets halfway through, because they may be taking a different test. I can take the compliance test really quickly or maybe they’re taking the CPC®-I test which is a 2-hour test. Don’t worry about anybody else testing, you pay attention to just yourself. Take a deep breath, you’re done. Walk out with all of your stuff, make sure you pick up your phone and then treat yourself. I always go and get ice cream after I have a test. But whatever you need to do, go home, have a glass of wine or whatever it takes to make you say, “Hey I did it” make your family take you out to dinner because you definitely not going to want to cook that night.
And So You Wait
Wait patiently. You’re going to get a notification in about 2 weeks. From now on to the end of the year, any time after July, it starts speeding up more people tests, so it slows down. But if you’re testing the first half of the year, then you could get your test results back in a week. You get them back even faster when you take it online.
Don’t even look for a week and then you log-in and if you passed, it will say, “you passed” and it will have your credential by your name, your new credential. If you did not pass, it will say “fail” and then you’re going to be able to click on that and it will give you a breakdown of your percentages for the test. But if you pass, you don’t get any of that information to see.
Again, just say, “I’m not going to look for an entire week.” And then I’ll go look. Then you’ll get an envelope from them with your credential and a bunch of nice plaques and some other things that they send you when you get another credential.
Alright guys, this has been a lot of fun. There are lots and lots of tips out there from people. The best thing you can do is just talk to other people that have tested and you’re going to do that by networking. You can talk to people online, you can talk to people in our CCO Club which they’ll be a link down below for that. What I want to encourage all of you guys to do is stay connected. We are on Facebook, we are on YouTube, we’re in LinkedIn, you can find me on LinkedIn and ask to connect via LinkedIn and then feel free to navigate through all the people that I’ve connected with.
These are the people that are going to help you get a job, these are going to be the people that are going to help you take other certification exams; you want to stay very connected to them.
In conclusion, these tips can be a great help in preparing for the CPC exam. AAPC provides reliable tips, and it’s essential to keep in mind the guidelines, organize your materials, and understand sequencing and additional notes. Take a course if you need to, refine and review your skills, and practice as much as you can. And remember, if you have any questions along the way, don’t hesitate to ask for help in the free CCO Community. Good luck on your certification journey!